
It's Grow Time
First week of IVF stims
After Erik and I made the decision to pursue IVF, we spent a little over one month on administrative prep work before we could actually begin treatment. Our fertility clinic first had to contact my insurance to confirm the specific procedures and costs covered by my healthcare plan. I must again express my gratitude to my employer for offering generous family-building benefits: a three cycle lifetime maximum toward fertility treatment and prescription injectable medication expenses. For reference, in Texas, one round of IVF, if paid for out of pocket, can cost between $10,000 and $30,000. I’m really thankful that finances was not a big factor in our IVF decision-making process. My insurance ended up approving the coverage of one egg retrieval cycle (to start), the associated embryo transfers, and up to one year of frozen embryo and/or egg storage. I was not eligible for PGT (preimplantation genetic testing) coverage, but it was okay as Erik and I had decided that we wouldn’t perform genetic testing on our embryos anyway.
Next, Erik and I had to sign consent forms. The document outlined the elements of IVF and their associated risks and then moved to disposition decisions—what to do with any cryopreserved embryos and eggs after a viable pregnancy is achieved. We went down the list of scenarios: death of the patient (me), death of the partner (Erik), death of patient and partner, the patient loses all ability to carry embryos, divorce, etc. We always chose the option that would preserve the embryos, whether it is giving to the other person or donating to another couple. The question that stood out was the one on divorce. The embryos could be given to the patient, given to the partner, or divided equally between patient and partner (the form even asks you to specify who gets the greater quantity if there is an odd number of embryos). At first we opted for equal division. But then we talked about how maybe I should get all the embryos, since I could transfer them into my own body while Erik would need to find a surrogate. Sitting on the couch, casually discussing what would happen to our hypothetical embryos in the event of our hypothetical divorce, was darkly humorous.
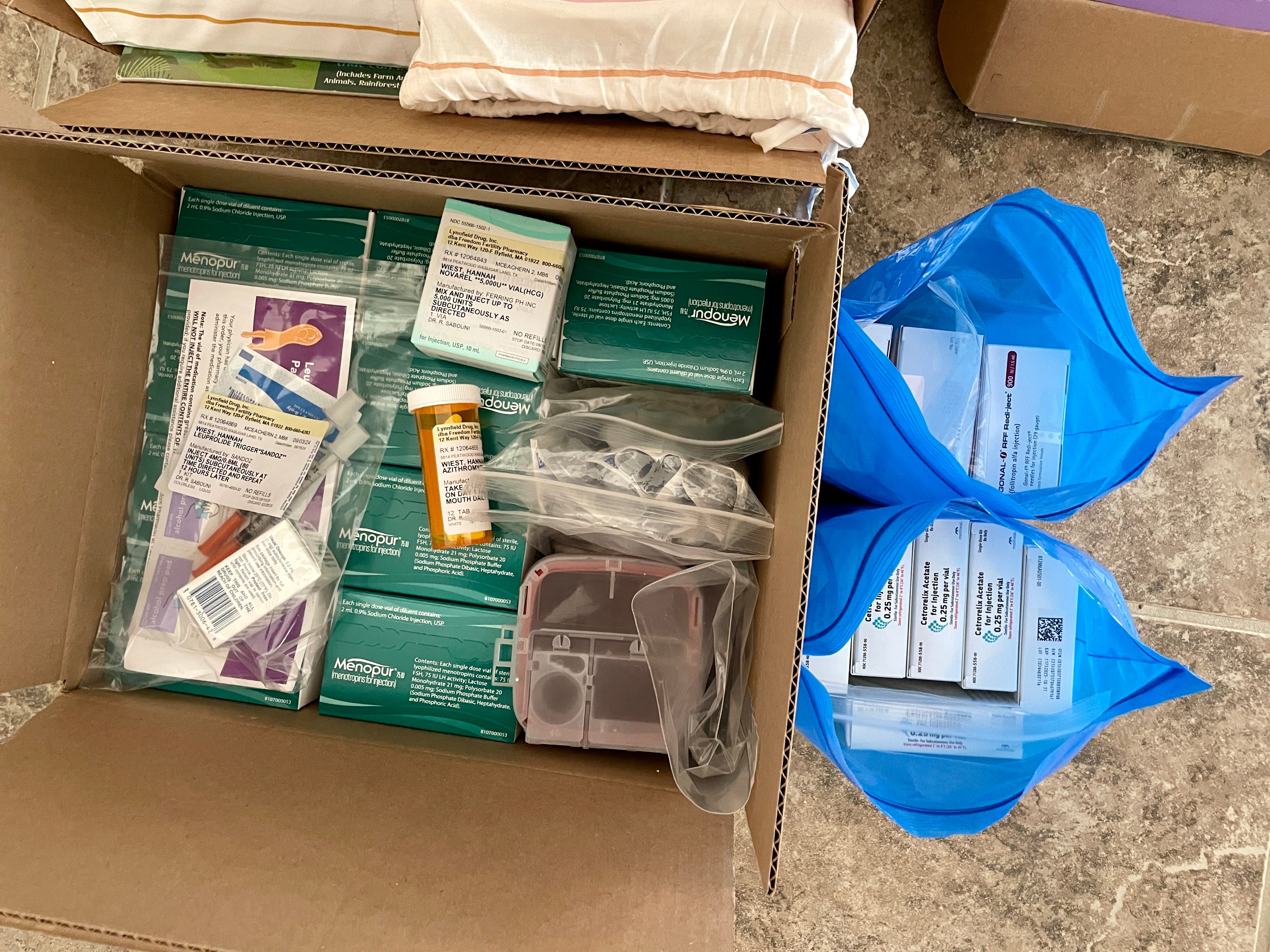
With the financing and consent forms taken care of, the fertility clinic placed an order for the ovarian stimulation medication. Although the specific medication protocol would not be determined until after my baseline appointment, I couldn’t schedule that appointment until I had received the medication. The medication order involved more bureaucratic red tape; I had a call with the pharmacy, who then contacted Cigna for approval and authorizations, after which the pharmacy called me again. A good portion of this whole IVF process is just waiting. When the pharmacy asked me what day I wanted the medication delivered, part of me wanted to start as soon as possible, but I went with wiser decision to wait until after my Florida vacation. The shipment arrived a few days after the trip, and the clinic scheduled my baseline appointment for several days after that.
At the appointment, they drew my blood to measure the levels of hormones such as progesterone, estrogen, LH (luteinizing hormone), and FSH (follicle-stimulating hormone), and I had an ultrasound to observe existing follicles in my ovaries and endometrial thickness. By that point, I had been on birth control for almost three months, so my hormone levels were low and my endometrium thin. In the event anything had looked off at the appointment, the start of ovarian stimulation would’ve needed to be delayed. (This is one of the many reasons it is hard to predict how long one cycle of IVF will take.) Fortunately, everything looked good, and I was instructed to begin injections on Friday, September 13th.
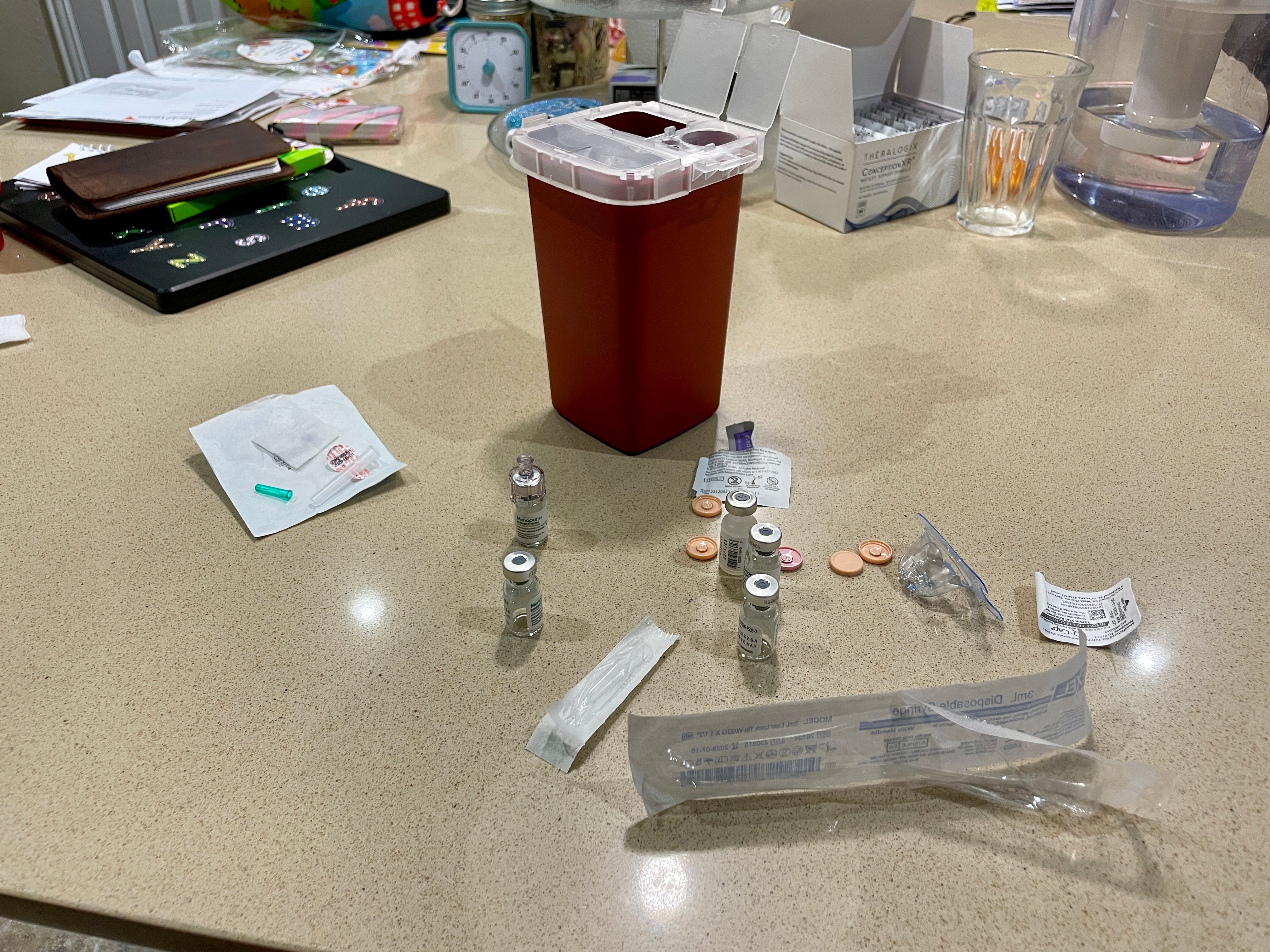
I am pretty okay with needles, but I think there is a big difference between being injected and injecting yourself. Luckily, Erik is also not very squeamish, so he agreed to do my injections. The day before we were scheduled to start, we watched multiple educational videos as well as YouTube vlogs of average people’s real-time experiences. My starting medication protocol was 225 IU of Gonal-F and 300 IU of Menopur. Gonal-F is a brand of FSH and comes in a “pen” form. You twist the top of the pen to the desired dose, insert the needle into your stomach, and press the top completely down (like clicking a pen) to inject the medication. Menopur is a brand of menotropins, a mix of FSH and LH. It is packaged as little vials of white powder. You use the provided sodium chloride to mix and dilute the powder. Injecting the diluent into the Menopur vial, swirling it around to dissolve the powder, then drawing everything back into the syringe—it feels like we’re in a chemistry lab!
Preparing the medication ourselves felt intimidating at first, but I reminded myself that tons of people go through IVF and have to do this, so surely we can do it, too. The injections also felt intimidating, but so far, one week in, they’ve been mostly fine. On the third night of stims, I did the injections myself. While I prefer that Erik does it, I need to be able to do it myself in the event he is unavailable, since the medicine needs to be administered at the same time every day. The feeling of the medication going into my stomach isn’t pleasant, and the injection site is a little sore afterward, but at least I haven’t experienced the burning sensation Menopur can have. As for side effects, the only one I’ve observed so far for me is mild headaches. I know the second half of the stims process is harder, though, as the amount of hormones adds up and the ovaries swell, so we’ll see.

After my baseline appointment, I scheduled follow-up appointments on the next Monday, Wednesday, and Friday for my doctor to check how my body is responding to the medication and if it is having the desired effect on follicle growth. At some point, I will add medication that prevents the LH surge that leads to ovulation. Basically, the ovarian stimulation process is a delicate balance of growing follicles while preventing premature ovulation. If, after 12-14 days of injections (though it could also be longer), there is a good number of good-sized follicles, the next step would be egg retrieval. With all of these doctor’s appointments, though each one doesn’t take long, I’m grateful for a flexible work schedule and understanding manager.
As of today, I’ve done seven days of injections and had three monitoring appointments. After the first one, my doctor increased my Gonal-F dose from 225 IU to 300 IU, and today I was instructed to add 0.25 mg of Cetrotide, the medication that delays ovulation, to the line-up. The follicles in my right ovary are not responding very much to the medication and are still small (<6 mm), but there are two good-sized follicles (~14 mm), among other smaller ones, in my left ovary. With my infertility diagnosis being DOR (diminished ovarian reserve), I don’t expect a high yield of eggs, but there will inevitably be some amount of disappointment if the egg retrieval is cancelled and we need to start over with stims or if we only retrieve a few eggs. But I came across John 14:27 twice in the past week, first in a missionary update email and then from someone I follow on Instagram, and it has been a comforting verse that I will continue to meditate on, whatever the outcome of this IVF cycle.
Peace I leave with you; my peace I give to you. Not as the world gives do I give to you. Let not your hearts be troubled, neither let them be afraid.